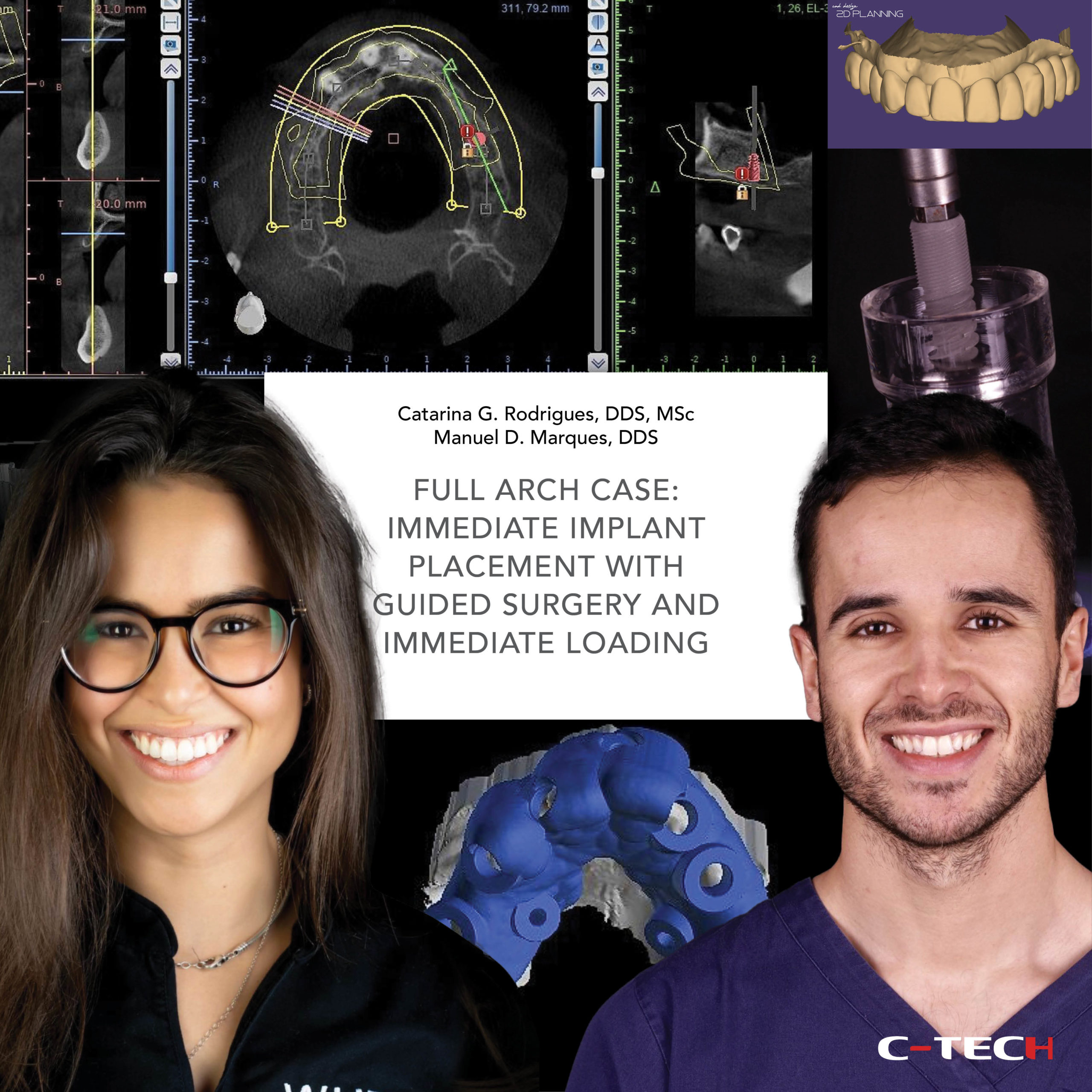
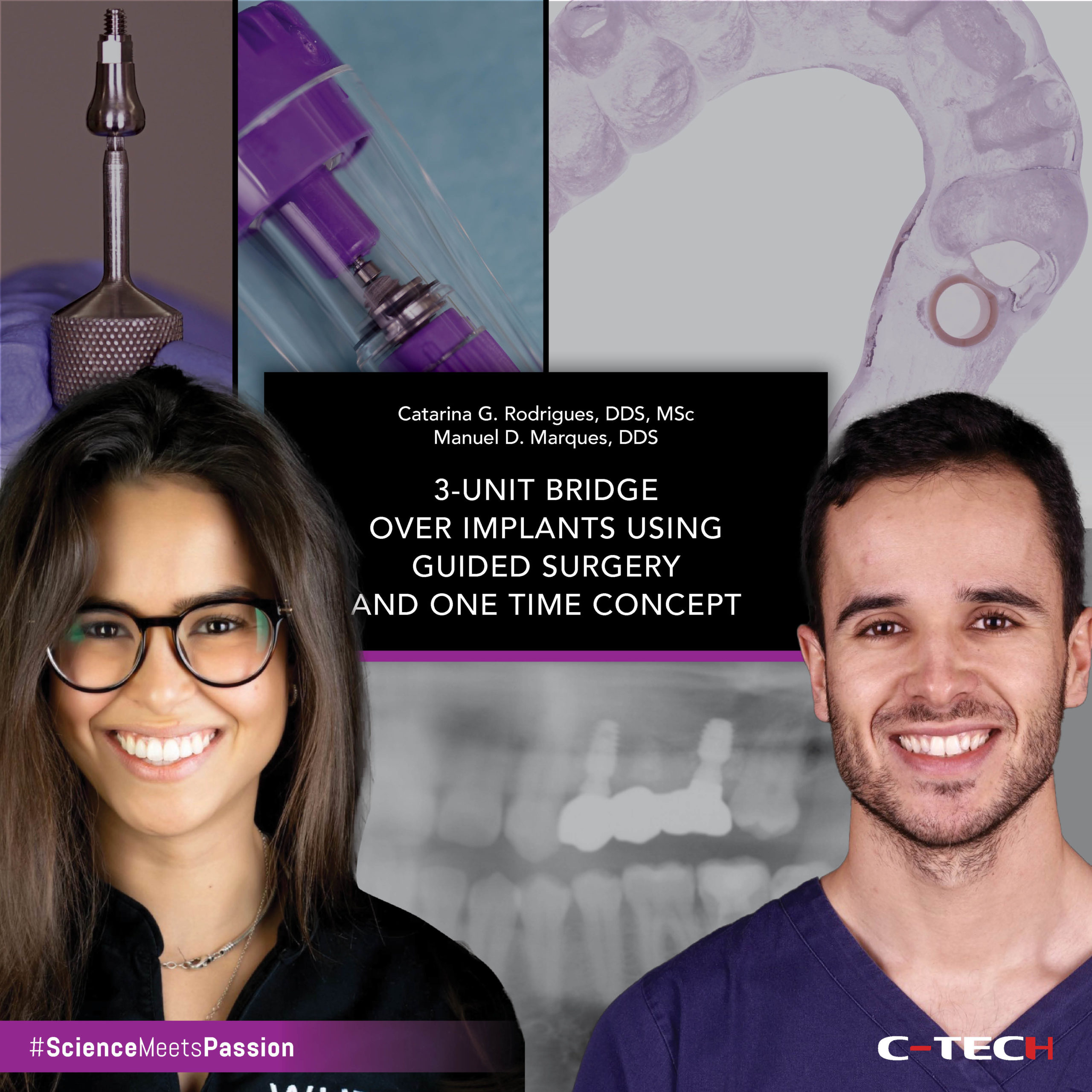
Dr. Catarina G. Rodrigues, DDS, MSc – Dr. Manuel D. Marques, DDS
A 50-year-old woman presented to a private practice very unhappy with the aesthetics of her smile. The patient said that her front teeth were always misaligned, but recently they had worsened considerably. In the initial extra-oral photographs we can note that the right central incisor is excessively inclined towards the buccal side and also extruded (Fig.1,2). 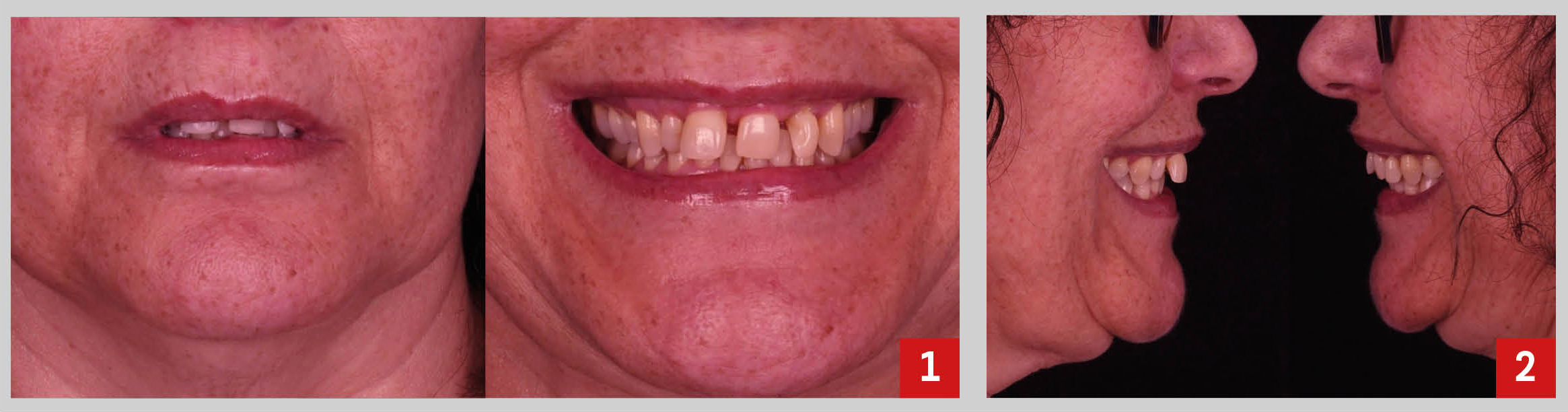
The initial intra-oral pictures revealed wrong tooth proportions and the presence of several spaces between the upper anterior teeth, which obviously compromised the aesthetics of her smile (Fig. 2-5). 
The radiographic examination revealed that the bone support of tooth 1.1 was very compromised. Also, clinically we detected grade II mobility (Fig. 6,7). 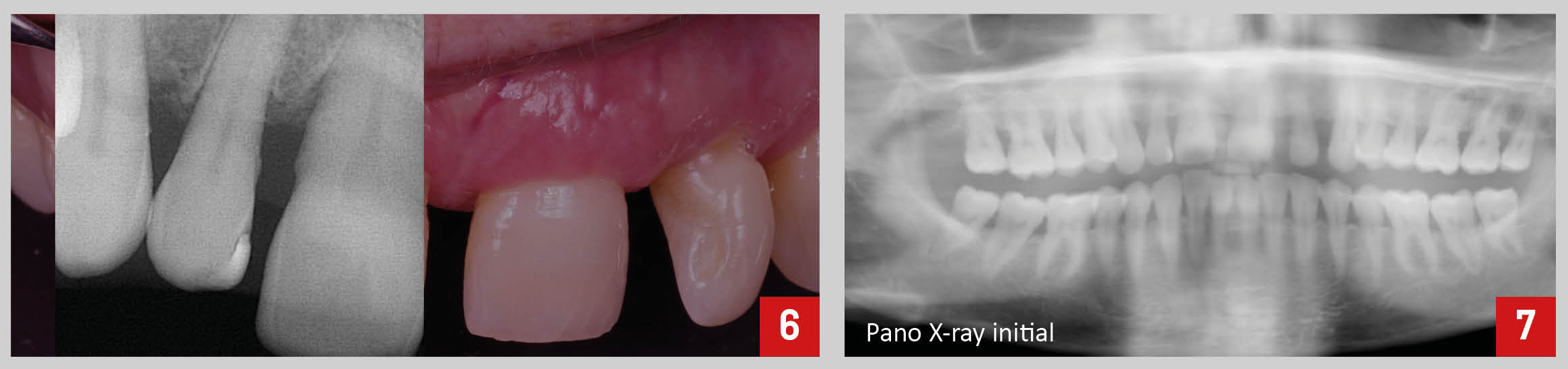
Following a proper diagnosis and given the fact that the patient asked for a minimal invasive approach, we proposed the following treatment plan: prophylaxis, direct composite restorations on teeth 1.2, 2.1 and 2.2, to help managing the interdental spaces and improve aesthetics, extraction of tooth 1.1 with immediate implant placement and immediate loading, and finally a ceramic crown over implant (Fig.8).
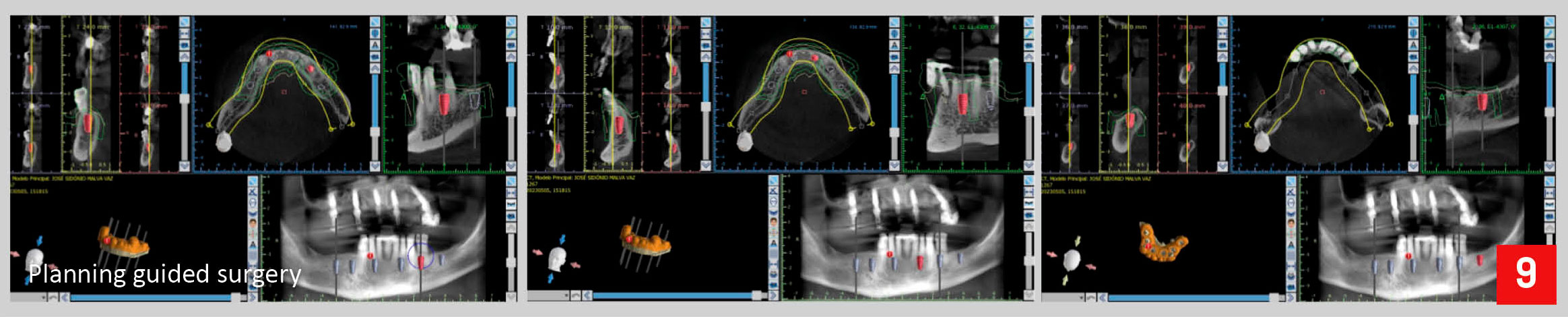
To perform a proper planning of the case, several records of the patient were obtained. Besides intra and extra-oral pictures, we did also full arch IOS impressions and CBCT (Fig. 9). 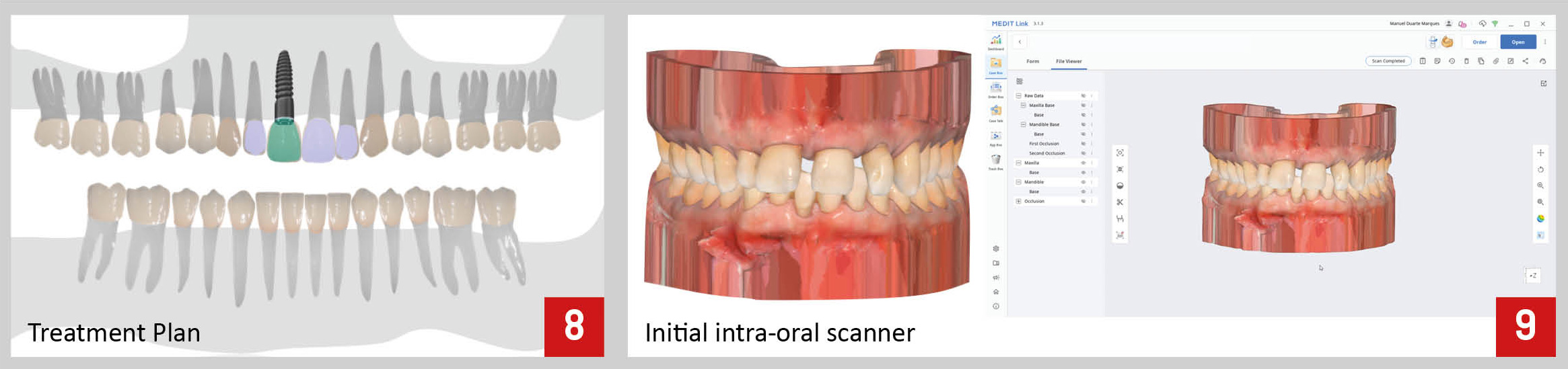
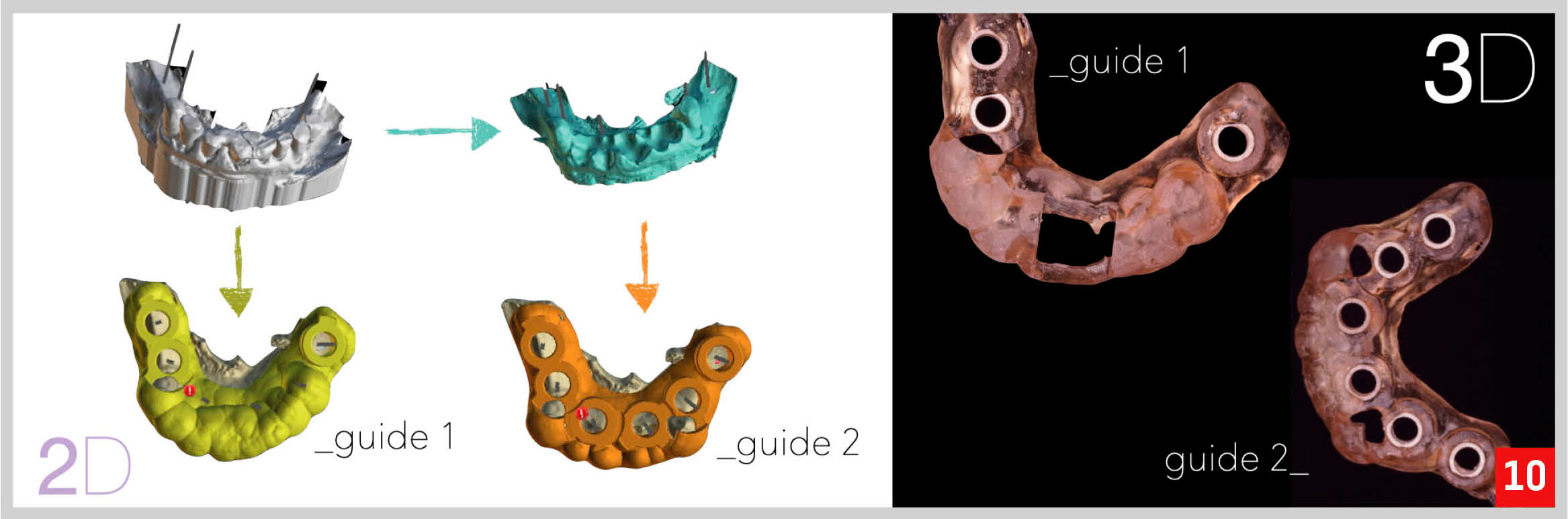
Since the original position of tooth 1.1 was not correct, this tooth was digitally extracted on the STL file and a 3D wax-up of a new central incisor with correct position, and proportions was digitally made to aid on the planning of the position and dimension of the future implant.
Then – using a specific software to plan the guided surgery – the STL files from the initial scan, the 3D wax-up and the CBCT were all superimposed, allowing the planning of the implant position accordingly to the planned future restoration (Fig.10). 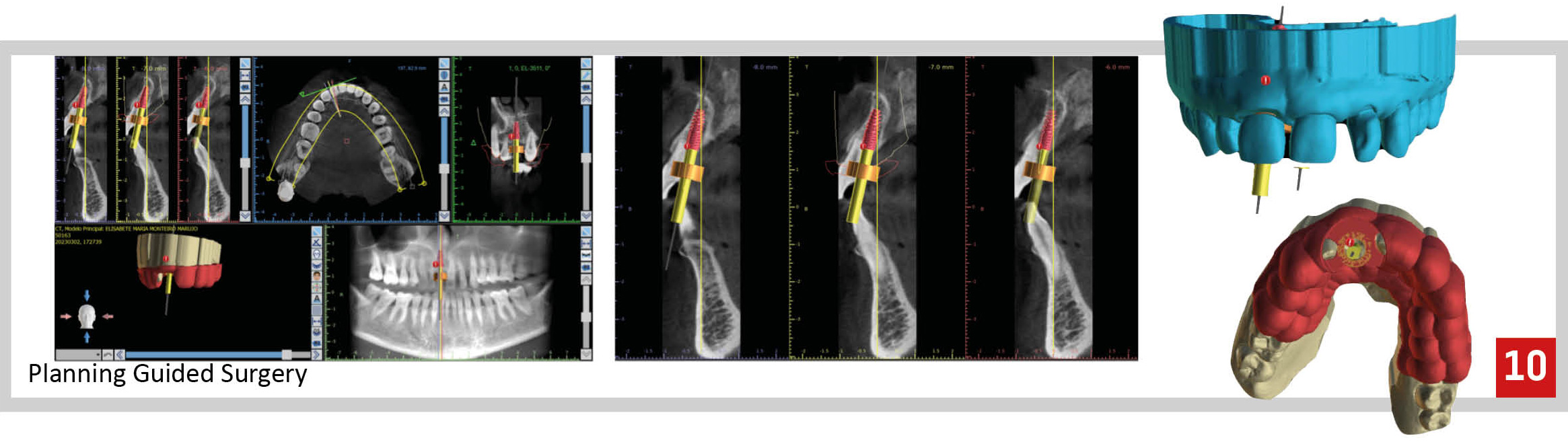
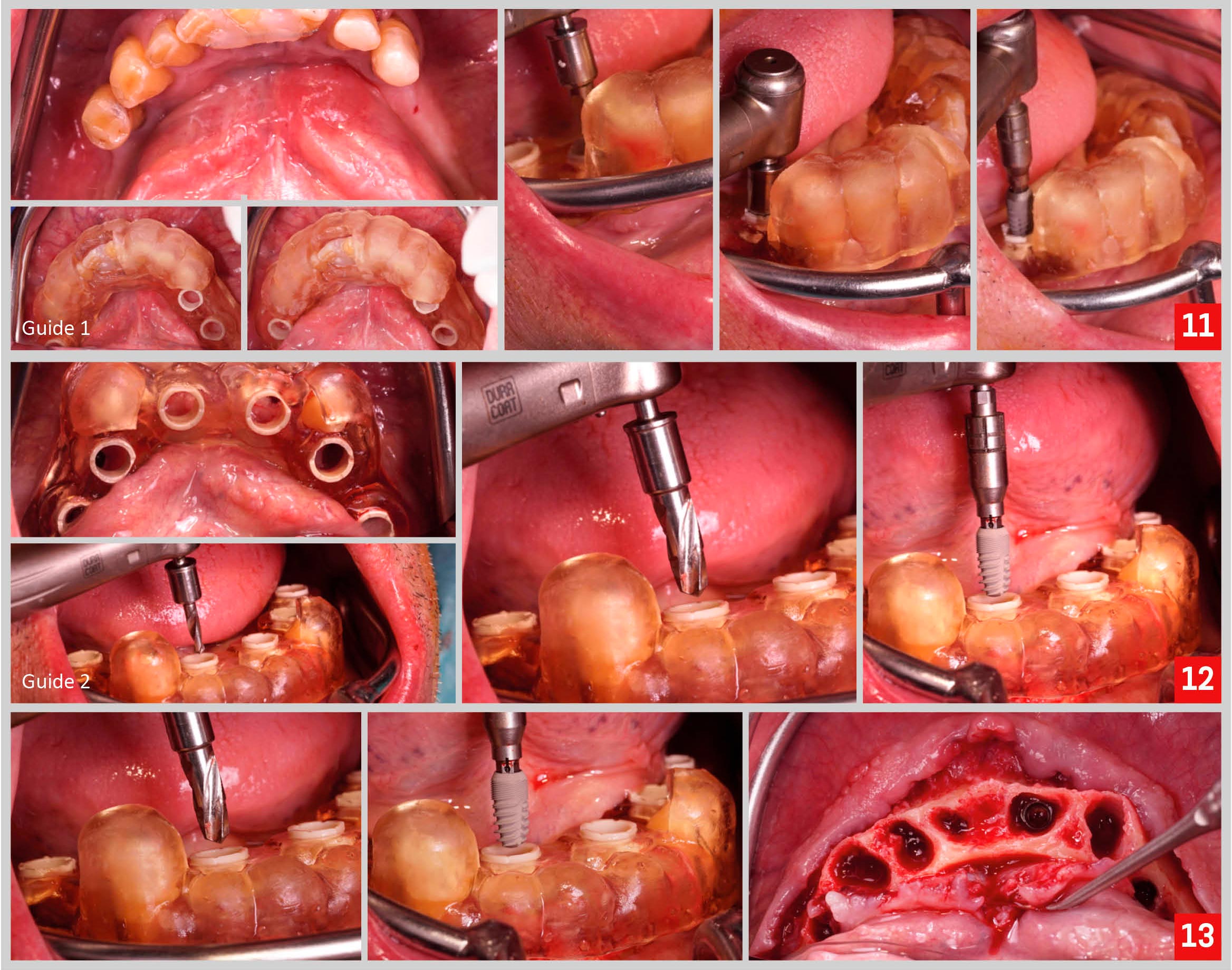
At the time of the surgery, tooth 1.1 was extracted using an atraumatic technique not to damage the bone or the soft tissues (Fig. 11,12). 
After that, the stability and adaptation of the guide were checked, followed by guided preparation of the implant site according to a specific drilling protocol and using C-Tech guided surgery kit. (Fig.13,14). 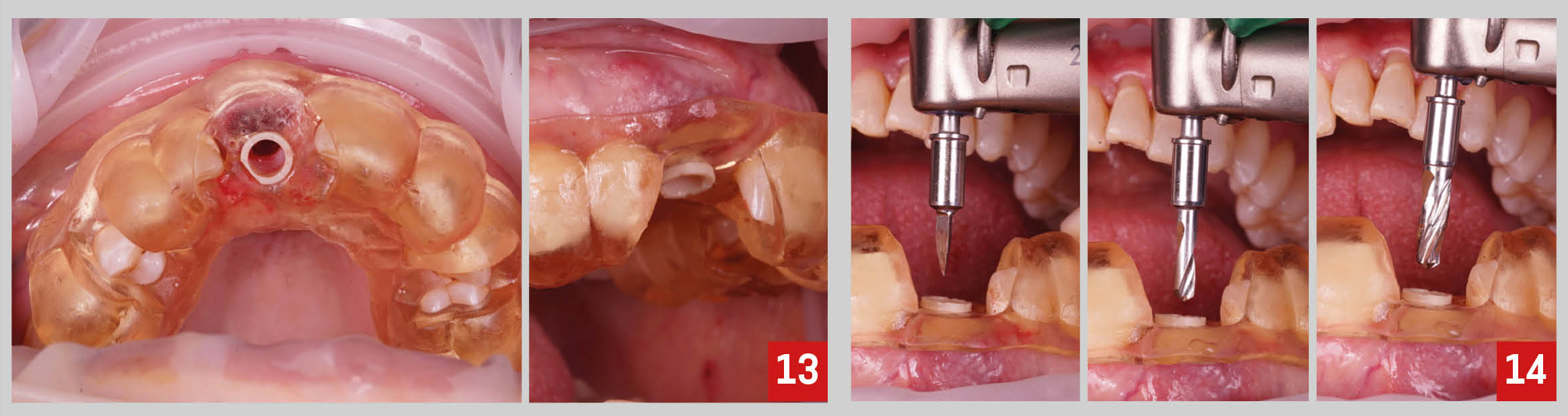
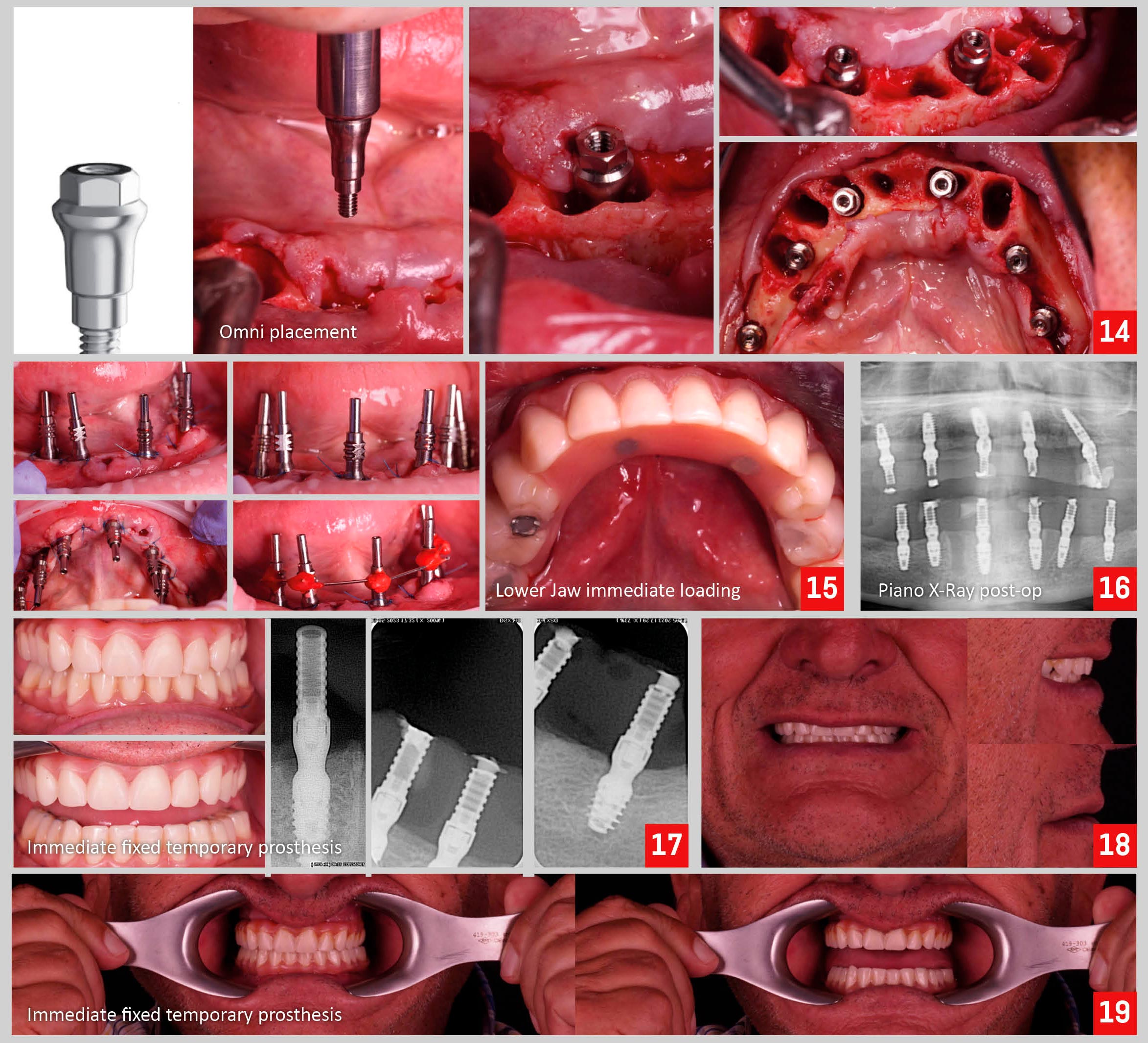
Finally, the implant was inserted through the guide and a connective tissue graft was preformed (Fig. 15-17). 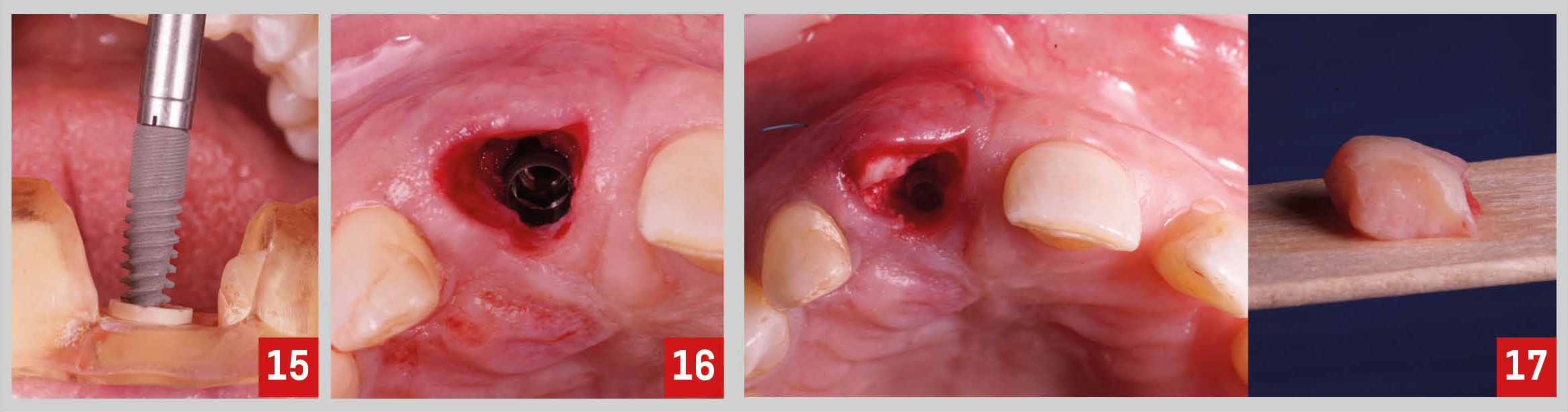
The immediate fixed provisional restoration was made with a titanium provisional abutment and the patient’s own tooth. The root of the extracted tooth was cut and prepared to be bonded to the titanium abutment. Then, the provisional crown was finished and polished (Fig. 18,19).
The 1-month follow-up appointment revealed very good healing and adequate aesthetics of the interim prosthesis. Also, on the periapical x-ray we can note the subcrestal position of the implant, ideal for the aesthetic zone once it allows proper emergence profile of the implant restoration and helps with long-term aesthetic stability (Fig. 20,21). 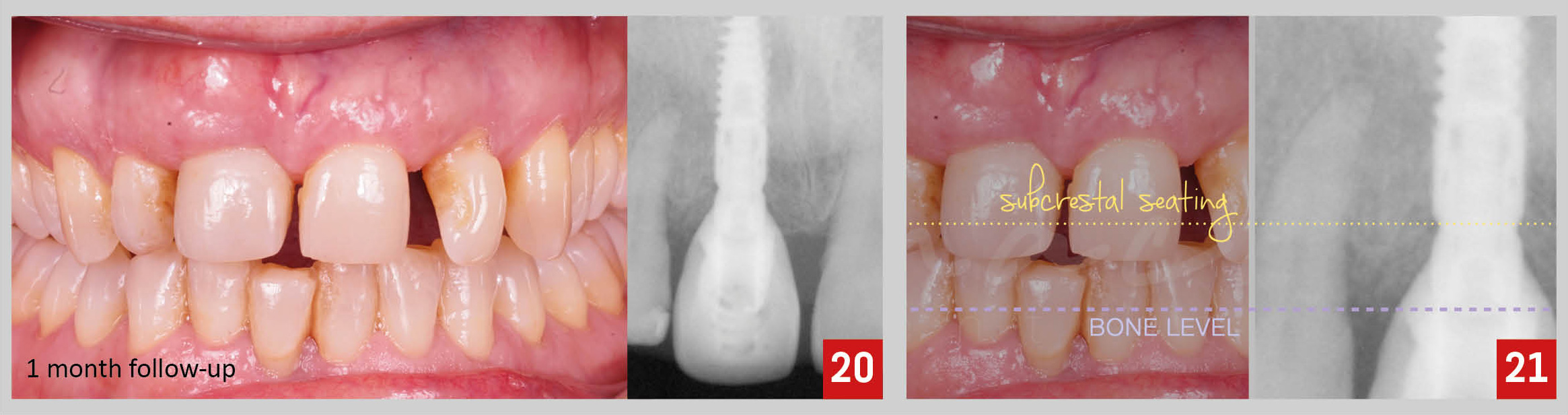
While we waited for the osseointegration of the implant, we proceeded with the direct composite restorations of teeth 1.2, 2.1 and 2.2. We selected the shade of the composite resin and then completed the direct restorations under rubber dam (Fig. 22-24). 
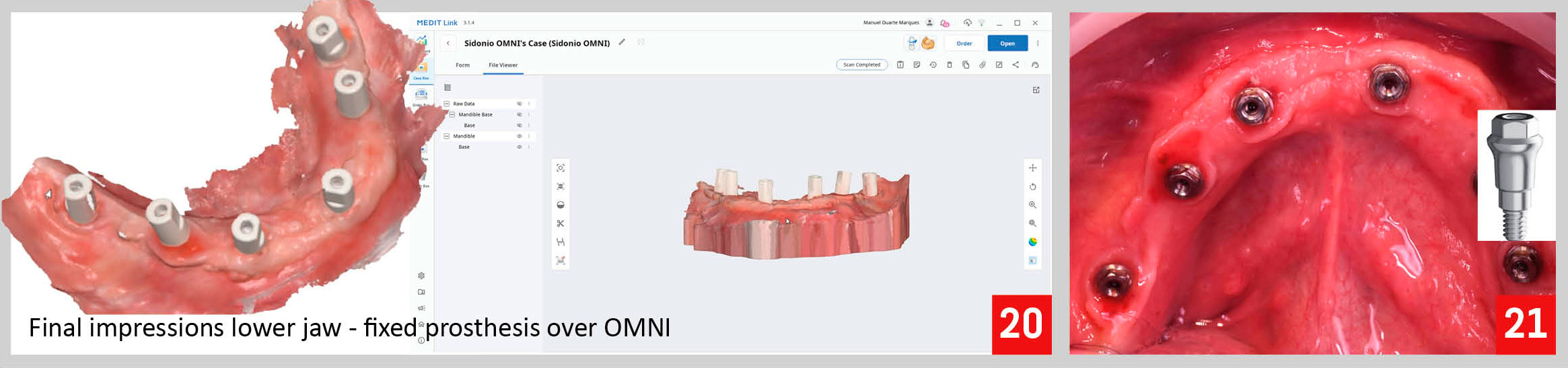
Later, 3 months after the implant surgery, we proceeded with the final impressions. To help the lab technician with the reproduction of the critical and subcritical contour of the provisional crown, I scanned first the provisional on the mouth and then the provisional crown alone (Fig 25). 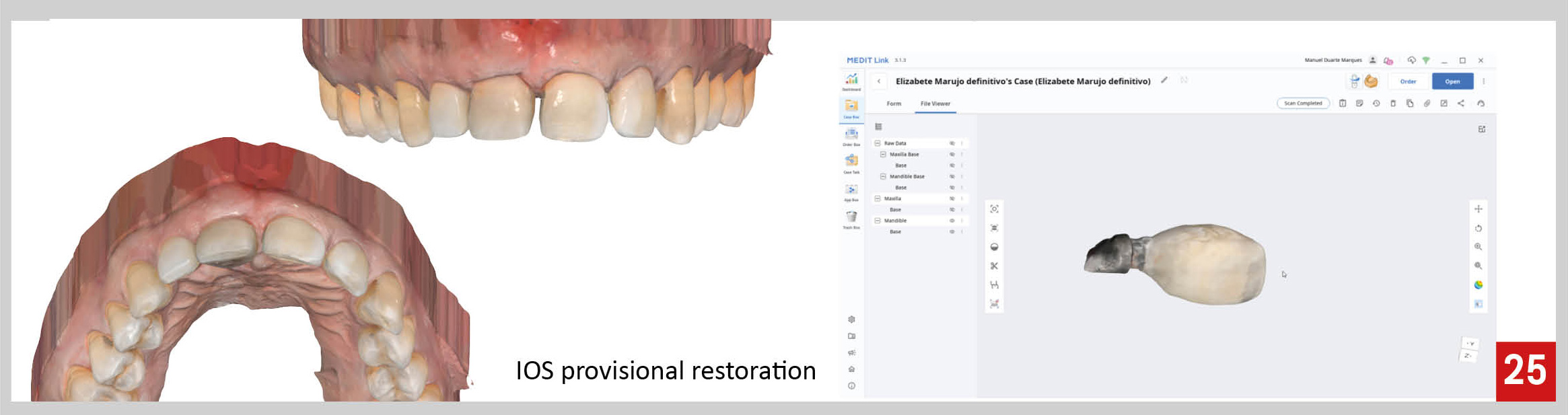
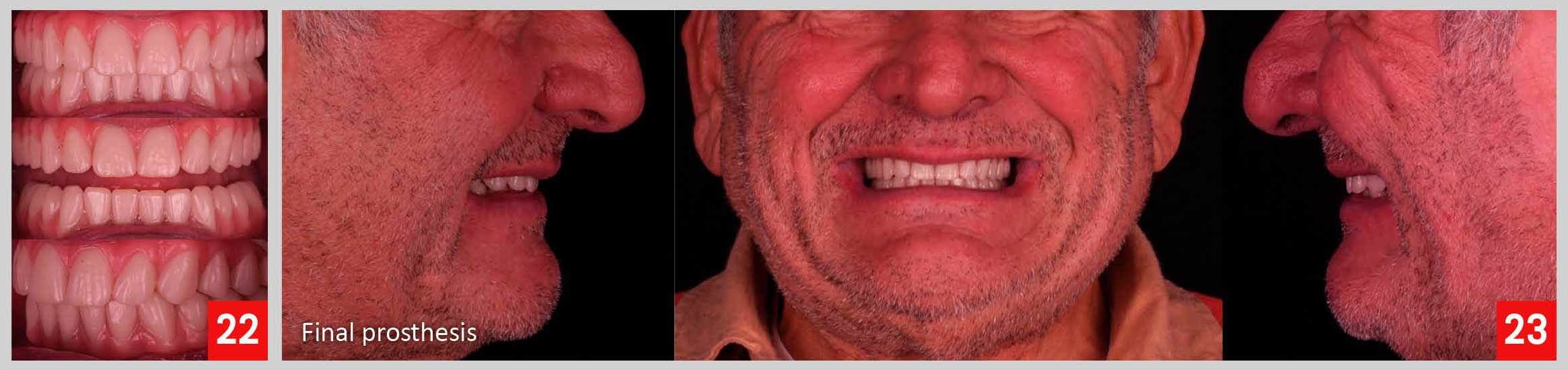
Finally we delivered the final restoration, a screw-retained layered zirconia crown over implant (Fig. 26-28).

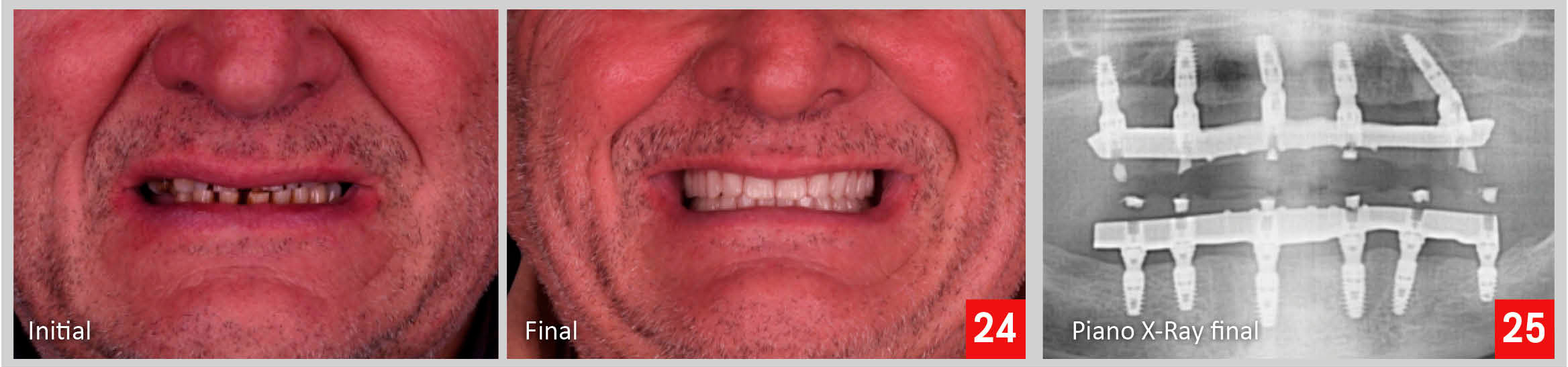
When comparing the initial situation of the patient and her final pictures, we can appreciate an important improvement on the aesthetics of her smile (Fig. 29-31).