
Full arch case: immediate implant placement with guided surgery and immediate loading
Catarina G. Rodrigues, DDS, MSc – Manuel D. Marques, DDS
A 57-year-old woman presented to a private practice with the chief complaint being “I’m self-conscious about the appearance of my teeth. Also, I’ve lost most of my teeth and I cannot eat well because of that”. The clinical and radiographic examination revealed the absence of all teeth except the central incisors and right lateral incisor in the upper. In the lower, partial edentulism, severe bone loss, and multiple periapical infections were diagnosed. Also, the patient’s function and aesthetics were seriously compromised (Fig 1-11).

Following a proper diagnosis, different treatment options to restore health, function, and aesthetics were considered and discussed with the patient. Finally, the chosen option was a two-phase treatment. Phase one consisted in extracting the remaining maxillary teeth and the lower ones that presented severe infection, placement of 6 implants on the upper with guided surgery, immediately provisionalization of the upper with a screw-retained acrylic prosthesis, and delivery of a provisional partial denture for the lower. Then, phase two, comprised of extraction of the remaining lower teeth, placement of 4 implants, followed by immediately provisionalization with a screw-retained acrylic prosthesis.
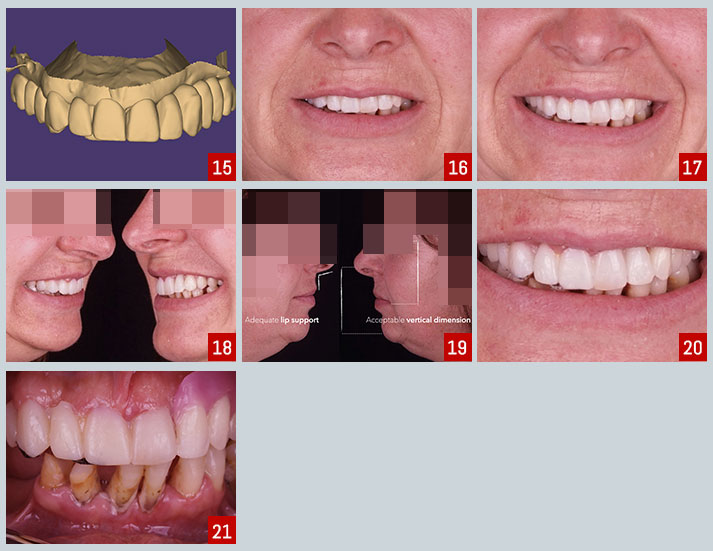
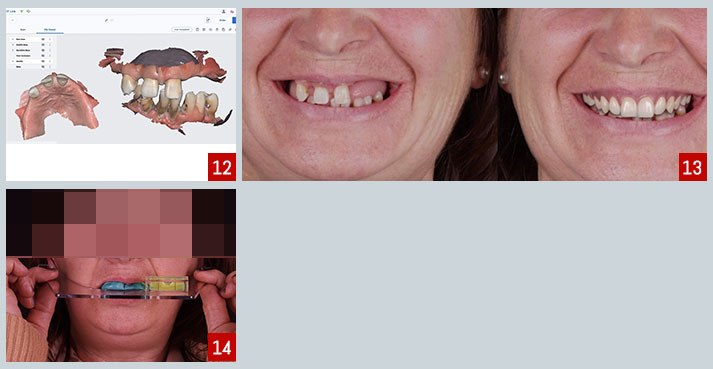 Multiple records of the patient were obtained in order to perform a proper planning of the case. Intra and extra-oral photographs, full arch IOS impressions (Fig.12) and CBCT. A 2D facially driven digital smile design was made to aid in the planning of the position and dimension of the teeth for the future interim prosthesis (Fig.13). The next step was pre-surgery prosthetic planning. In this case, a maxillary orientation silicone key was used to obtain an adequate position of the maxillary in a 3-dimensional space and to record the occlusal plane (Fig.14). This technique provides a method of virtually mounting the maxillary scan and transferring both the functional and the esthetic occlusal reference plane in a digital workflow. Using the previously made 2D smile design and the references recorded on the maxillary orientation silicone key, a try-in of the future interim prosthesis was created (Fig. 15-21).
Multiple records of the patient were obtained in order to perform a proper planning of the case. Intra and extra-oral photographs, full arch IOS impressions (Fig.12) and CBCT. A 2D facially driven digital smile design was made to aid in the planning of the position and dimension of the teeth for the future interim prosthesis (Fig.13). The next step was pre-surgery prosthetic planning. In this case, a maxillary orientation silicone key was used to obtain an adequate position of the maxillary in a 3-dimensional space and to record the occlusal plane (Fig.14). This technique provides a method of virtually mounting the maxillary scan and transferring both the functional and the esthetic occlusal reference plane in a digital workflow. Using the previously made 2D smile design and the references recorded on the maxillary orientation silicone key, a try-in of the future interim prosthesis was created (Fig. 15-21).
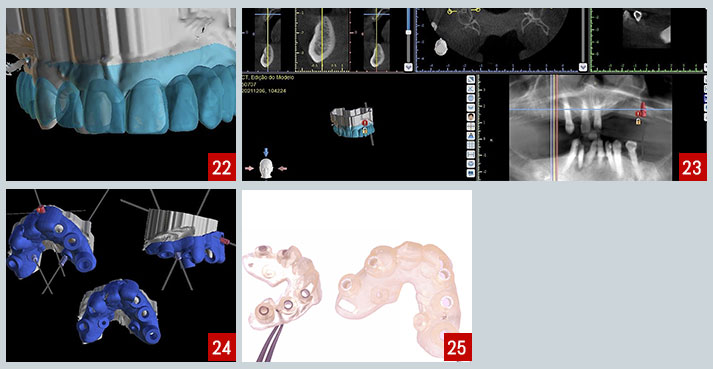
 The approved teeth try-in was then superimposed with the preoperative intra-oral scan and CBCT using an implant planning software. After this step, the actual process of prosthetic-driven implant planning started (Fig.22,23). After the implant planning has been finalized and approved, the surgical guide was designed using the same software (Fig.24). The multi-unit abutments for the upper jaw were also planned in advance. Finally, the guide was 3D printed (Fig.25).
The approved teeth try-in was then superimposed with the preoperative intra-oral scan and CBCT using an implant planning software. After this step, the actual process of prosthetic-driven implant planning started (Fig.22,23). After the implant planning has been finalized and approved, the surgical guide was designed using the same software (Fig.24). The multi-unit abutments for the upper jaw were also planned in advance. Finally, the guide was 3D printed (Fig.25).
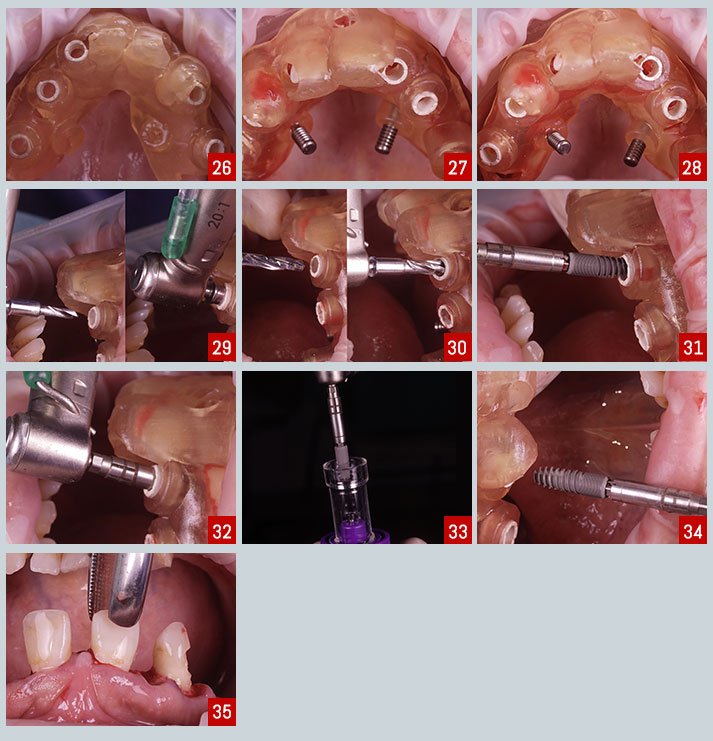
 At the time of implant surgery, the stability and adaptation of the guide were checked, followed by guided preparation of the implant sites according to a specific drilling protocol and using C-Tech guided surgery kit. Two fixation pins were placed to increase the stability and precision of the guide (Fig. 26-35).
At the time of implant surgery, the stability and adaptation of the guide were checked, followed by guided preparation of the implant sites according to a specific drilling protocol and using C-Tech guided surgery kit. Two fixation pins were placed to increase the stability and precision of the guide (Fig. 26-35).
 Multi-unit abutments were seated on the implants and immediately loaded with a screw-retained prosthesis (36-40).
Multi-unit abutments were seated on the implants and immediately loaded with a screw-retained prosthesis (36-40).
 The 2-week follow-up appointment revealed good healing and adequate function and aesthetics of the interim prosthesis (Fig.41,42).
The 2-week follow-up appointment revealed good healing and adequate function and aesthetics of the interim prosthesis (Fig.41,42).