
Mini Implant Guided Surgery, Full edentulous mandible prosthesis stabilized transgingivally in under an hour – clinical case
Dr. Alexandre Minis, France
Case description
68-year-old man, fully edentulous, smoking patient, lack of medical history.
Surgical dental history:
– maxillary rehabilitation by full implant-supported bridge
– failure of 2 mandibular implant surgeries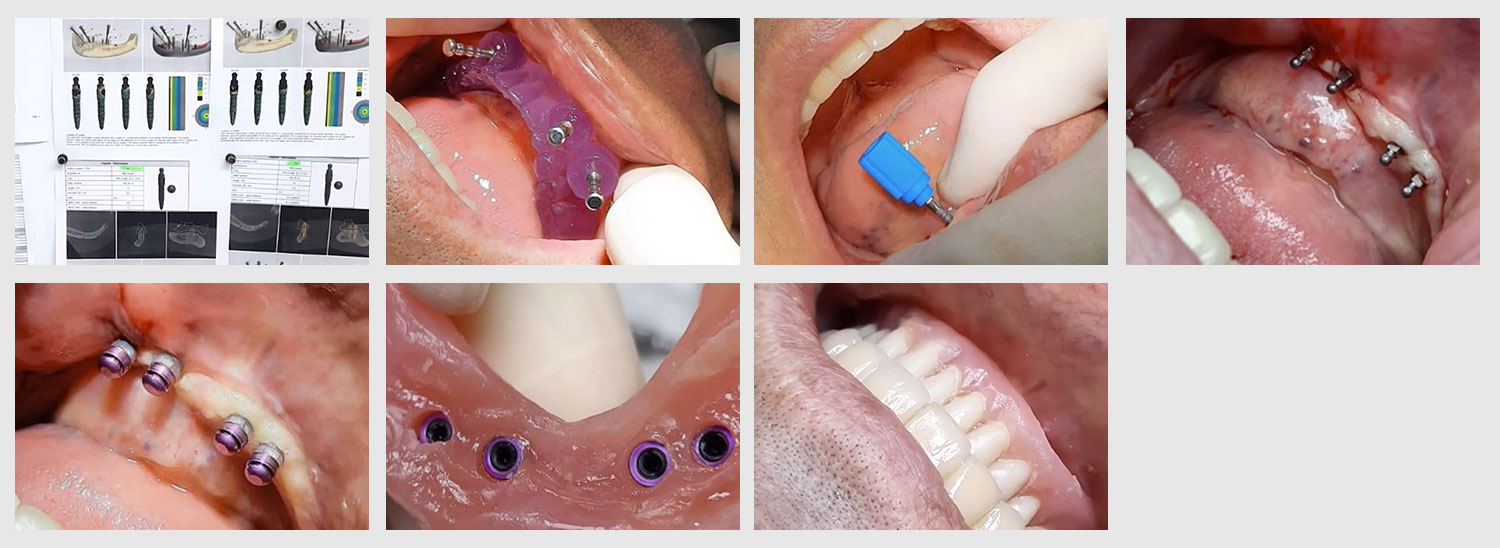
Limited quantity of mandibular bone, in fact the mandibular nerve runs along the edge of the bony crest from the mental foramen. It was impossible to place posteriorly without a complex graft with displacement of the mandibular nerve. In addition, the patient did not want an invasive procedure and wanted to return to normal eating habits as soon as possible without waiting for an extended healing period. The choice of guided surgery combined with mini implants meant less bone volume was required and despite the lacking volume the procedure could be performed flaplessly and thus improve the patients healing period and decrease post operative discomfort.
Our choice therefore was for the placement of 4 X 2.4mm diamter x10mm length, agressive thread mini dental implants.
To ensure the chances of success, the patient was convinced to cease smoking 1 month prior to implantation.
The guided surgery was performed using a surgical guide, designed on 3Shape Implant Studio using the double scan technique. The surgical guide was printed on a Phrozen Shuffle printer.
The implants were planned intra-foraminally and satisfactory primary stability of over 35ncm was achieved on all implants. Accordinging to this initial stability, the patient could return to normal eating habits the same evening of the operation.
To minimize costs the patient’s existing prosthesis could be used with recess in the prosthesis at the location of the implants . Housings were placed over the implants with the protective sheaths directly in the mouth. The Pick up technique was performed using an hard pick up material. Verification of the occlusion was made once the caps were blocked, then the classic finishing / polishing is carried out. As we reused the patient’s prosthesis and always with the objective of maximizing the chances of success, relining was done immediately in order to balance the support points of the prosthesis.
The patient was back home 90 minutes after the start of the surgery. He will be followed up after 10 days.
The maintenance of the O-Ball abutments is essential for therapeutic success, the patient is therefore invited to maintain them with a soft manual brush.