Doctor Peng Dong, the expert of tooth implantation in Peking University International Hospital and president of Beijing Hedu Stomatological Clinic Co., Ltd
Medical Case Report
| Sex / Age: Female/37 |
|
| First Visit: 09/01/2014 |
Implant Surgery: 24/05/2018 |
| Others Surgery (GBR…): 26/10/2017 |
Final Restoration: 11/10/2018 |
| First Recall: 18/10/2018 |
|
| Chief Complaint: The patient seeks medical consultation for a loose maxillary tooth that was interfering with eating. |
| Consideration(s): Immediate implantation + Immediate extraction + Maxillary Sinus Lift + GBR |
CASE OUTLINE
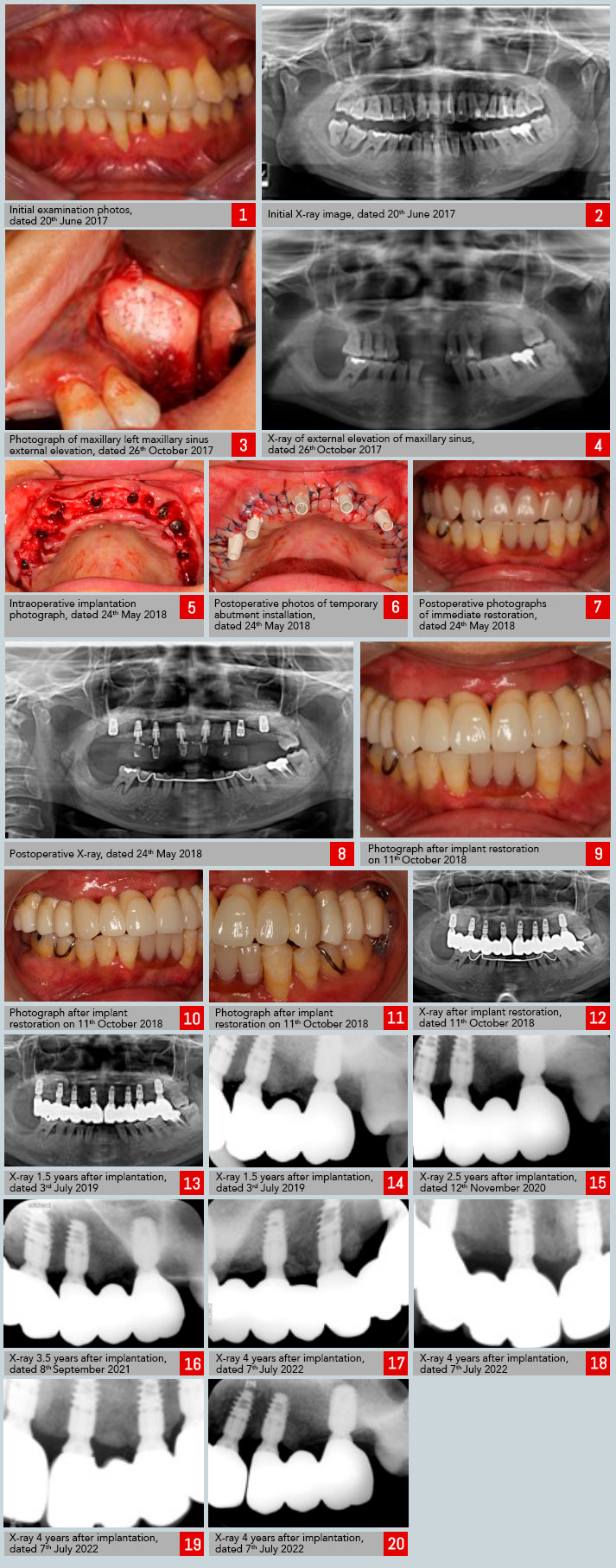
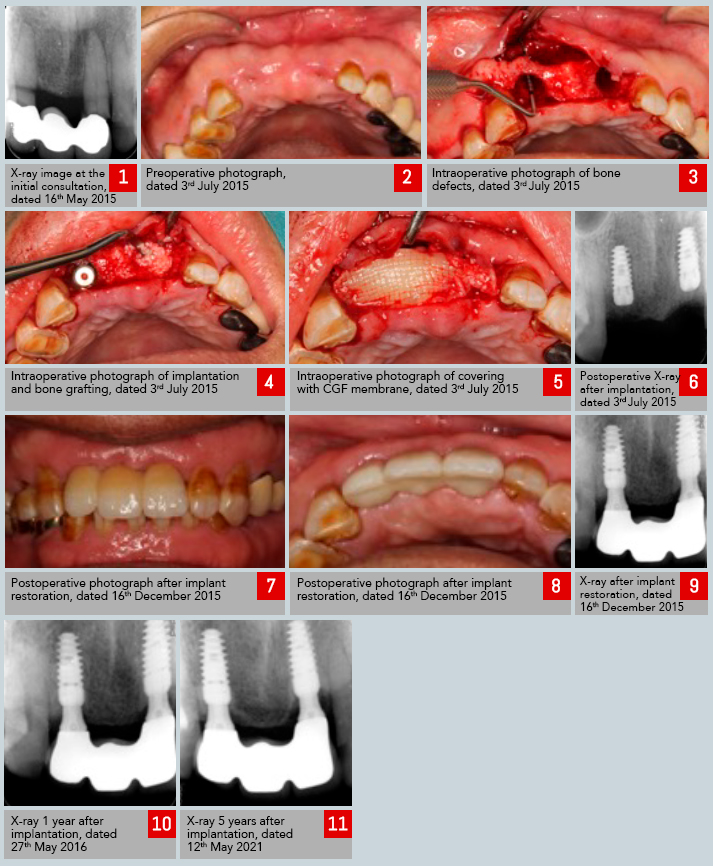
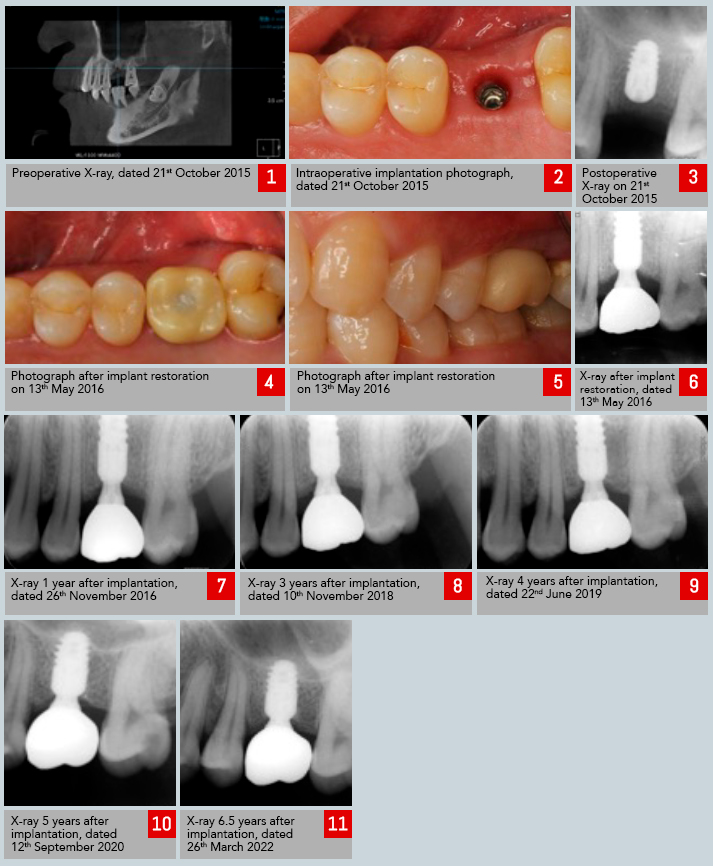
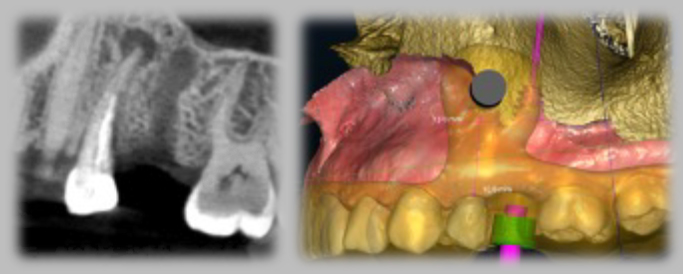
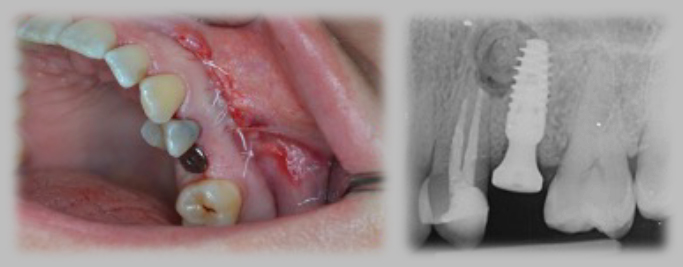
Significant absorption of the alveolar bone of the upper teeth is observed, with a large area of periapical radiolucency and root absorption reaching one-third to one-half of the length of the root. The diagnosis is invasive periodontitis. After a maxillary sinus lift procedure, the affected teeth were extracted, and immediate implantation of a total of eight C-Tech implants (Models: EL-3509, EL-4309, EL-5109) was performed. Subsequently, an oxidized zirconia full crown bridge will be used for restoration.
TREATMENT PLAN
After a maxillary sinus lift procedure on both sides, with the alveolar bone width being ideal but lacking in height, the affected teeth will be extracted. Subsequently, immediate implantation of eight C-Tech implants (Models: EL-3509, EL-4309, EL-5109) will be performed. At the same time, bone grafting will be conducted to support the implants, and a fixed temporary denture will be placed, supported by the implants.
TREATMENT
1. Perform standard disinfection and drape the area with cloths. Administer local infiltration anesthesia to the maxillary operative site.
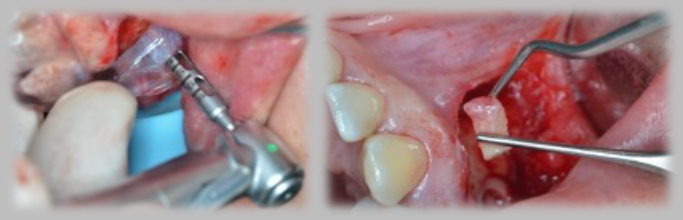
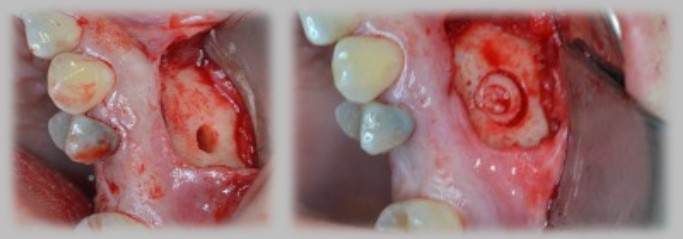
2. Perform a slanted incision in the upper right tooth 7, vertical incisions in the upper right teeth 6, 5, 4, and 3, internal incisions in the upper right second molar to the upper left teeth 2 to 1, and internal incisions in the upper left teeth 2, 3, and 4, and an internal incision in the upper left teeth 5, 6, and 7, and an internal incision in the upper left tooth 8. Elevate the flaps to expose the bone surface, remove the upper right teeth 6, 5, 4, and 3 and the upper left teeth 2, 3, and 4 with forceps, thoroughly cleanse the sockets, and use bone rongeurs and large round burs to carefully smooth and level the bone surface.
3. In the upper right tooth 1, prepare a borehole with a tapered drill and compress the bone to achieve a borehole size of 3.0*11mm. Implant a C-Tech implant (Model: EL-3509) with a PEEK base (Model: EL-4504P) at a torque of 45N. The marginal bone height is M1.5D1.5B1.5L1. In the upper right teeth 3, 1, and 3, prepare boreholes with tapered drills and compress the bone to achieve a borehole size of 3.0*11mm. Implant C-Tech implants (Model: EL-3509) with PEEK bases (Model: EL-4504P) at a torque of 45N. The marginal bone height for the left first molar (tooth 1) is M2.5D2B1.5L2, M1.5D1.5B-1.5L1.5 for the left third molar (tooth 3), and M2D1.5B2L1.5 for the right third molar (tooth 3). In the upper right tooth 4, prepare a borehole with a tapered drill and compress the bone to achieve a borehole size of 3.8*11mm. Implant a C-Tech implant (Model: EL-4309) with a PEEK base (Model: EL-4504P) at a torque of 45N. The marginal bone height is M1.5D2B1.5L1.5. In the upper left tooth 4, prepare a borehole with a tapered drill to achieve a borehole size of 3.8*11mm. Implant a C-Tech implant (Model: EL-4309) at a torque of 10N. The marginal bone height is M1.5D-8B1.5L1.5. In the upper right and left teeth 6, prepare boreholes with tapered drills to achieve a borehole size of 3.8*11mm. Implant C-Tech implants (Model: EL-5109) with cover screws. The marginal bone height for the left tooth 6 at a torque of 25N is M1D1B1.5L0.5, and M1.5D1.5B1.5L1.5 at a torque of 45N for the upper right tooth 6. Place Bio-Oss bone powder in the bone defects around the upper right teeth 3, 1, and left teeth 1, 3, 4 and the lip-side bone plate. Cover the bone grafting areas with membranes. Similarly, apply over the extraction site of the upper right tooth 6. Close the incisions with interrupted sutures to promote healing.
4. Use temporary abutments on the upper right teeth 4, 3, and 1 and the upper left teeth 1 and 3 to fabricate immediate upper dentures, adjust the occlusion, and polish the prosthetics.
5. After 9 months, take an impression, replace the restoration abutments, fix them with adhesive bonding, and provide permanent restoration with zirconia porcelain crowns and bridges. Left