Emerging Trends in Oral Health Sciences and Dentistry • 2015
Narrow Diameter and Mini Dental Implant Overdentures
Introduction
Complete dentures are most frequently a challenge for practitioners. The complexity of this disease is often associated with general health problems, but also with the physiological ageing phenomenon, that increases the treatment difficulty. Completely edentulous patients, usually elderly, often complain about the functionality of conventional dentures, especially the mandibular ones, claiming their instability, poor retention and discomfort during wear. Complete maxillary and mandibular dentures have been for over 100 years the standard treatment of complete edentulism. If complete maxillary denture wearers tolerate better the complete dentures, given the better conditions for support, retention and stability, the tolerance of mandibular prosthesis is generally lower. The relatively frequent instability of the mandibular denture, poor retention and associated discomfort were the starting point for the idea of setting the overdenture on 2 implants as first treatment alternative for the mandibular complete edentulism (according to McGill and York consensus) [2, 3, 4].
Concept of implant overdentures
Implant overdentures are inspired, as treatment concept, from the of the overdentures, the dental implants being used instead of tooth roots. Dental implants that are used for implant overdentures are made of high-strength alloy (TiAl-V), with good biocompatibility, with different designs and sizes that aim to address the prosthetic needs according to the oral particularities and clinical limitations of its execution. The first implants that were introduced in the dental practice were the ones with standard diameter, around 3.75mm. Later on, their diameter was increased and decreased (narrow), ranging between 3 and 6mm. Afterwards, the mini implants with one-piece design for implant overdentures appeared (IMTEC, later 3MESPE), with diameters of 1.8mm, 2.1mm and 2.4mm. Narrow Diameter Implant Overdenture (NDIO) represents a category of implants that combines features from conventional implants and mini implants, with diameters between 3 and 3.5mm and variable lengths (10-18mm), comprising two distinctive subgroups, namely two-piece design (e.g. Seven Narrow Line implants, MIS Implants Technologies Inc. 18-00 Fair Lawn Ave. Fair Lawn, NJ 07410, UNITED STATES, mini Sky 2, Bredent Medical GmbH & Co, Germany, Straumann implant, Straumann Group SIX: STMN, Basel Switzerland) and one-piece design (e.g. uno line, MIS implants). Two-piece narrow implants can be used as the conventional implants (with delayed loading), or as one-piece mini implants (with immediate loading protocol). In relation to anatomical, functional and prosthetic case particularities, the number of dental implants used can be reduced, similar to that of the conventional implants (e.g., two narrow implants for the mandibular overdenture). Mini Dental Implant Overdentures (MDIO) use mostly-one piece dental implants (miniSky1, Bredent, MDI 3MESPE) with diameters between 1,8mm and 3mm and variable lengths (10mm-18mm), that require one-stage surgery for implant placement, followed by prosthesis application in the same appointment, with soft material in the housing area (progressive loading) or fixation of the matrices in the denture base (immediate loading). Within the mini implants, those with a diameter between 2.7 and 3mm are classified as hybrid implants, these having sometimes a two-piece design and can be used as narrow dental implants (e.g., two narrow implants for the mandibular overdenture). The main features of the overdentures on dental implants with a diameter below the conventional one, considering their three main categories according to their diameter, are synthesized in table 1. The decision to use either a CDIO, NDIO or MDIO as treatment for complete edentulism, starts from the acknowledgment of patient’s preferences and expectations, within the limitations of the systemic and oral health-status. In systemic alterations with indications of limited surgery or that negatively affects the healing process, NDIO and MDIO are more indicated than CDIO, due to their reduced invasiveness. Oral particularities, such as the anatomical conditions (bone quality and quantity, the shape of the alveolar ridge, skeletal class), thickness and health of the oral mucosa (e.g., denture stomatitis, candidiasis), available prosthetic restorative space (especially as vertical dimension, given the necessary space for abutment, attachments and prosthesis thickness, in order to prevent its fracture) should all be considered when choosing between the implant prosthesis alternatives.
Conclusions
Stabilization of conventional denture with mini- or narrow-dental implants is beneficial especially for the elderly, considering the improvement achieved through a relatively easy surgical intervention, with moderate treatment costs. In this regard, for mandibular denture stabilization either 4 mini implants or 2 hybrid/narrow implants can be used. Treatment success is strongly related to acknowledgement of patient anatomical and functional particularities, rigorous planning and execution of prosthetic and surgical phase, as well as ensuring an adequate maintenance. Considering that edentulism is and most probably will continue to remain a frequent medical condition mostly found in the elderly, MDIO and NDIO overdentures, through their specific parameters, may replace in time complete dentures and may be the most used treatment alternative.

References
[1] WHO. Active Aging. A Policy Framework. Madrid; 2002. http://whqlibdoc.who.int/hq/2002/WHO_NMH_NPH_02.8.pdf?ua=1 (accessed 3 October 2014).
[2] Thomason JM, Kelly SA, Bendkowski A, Ellis JS. Two implant retained overdentures–a review of the literature supporting the McGill and York consensus statements Journal of Dentistry 2012;40(1) 22-34..
[3] Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, Head T et al. The McGill Consensus Statement on Overdentures. Montreal, Quebec, Canada. May 24-25, 2002. International Journal of Prosthodont 2002;15(4) 413-4.
[4] Melescanu Imre M, Marin M, Preoteasa E, Tancu AM, Preoteasa CT.Two implant overdenture–the first alternative treatment for patients with complete edentulous mandible. Journal of Medicine and Life 2011;4(2) 207-9.
[5] Preoteasa E, Marin M, Imre M, Lerner H, Preoteasa CT. Patients’ Satisfaction With Conventional Dentures and Mini Implant Anchored Overdentures. Revista MedicoChirurgicala a Societatii de Medici si Naturisti din Iasi 2012;116(1) 310-16.
[6] Klein MO, Schiegnitz E, Al-Nawas B. Systematic review on success of narrow-diameter dental implants. The International Journal of Oral & Maxillofacial Implants 2014;29 Supplement 43-54.
[7] Diz P, Scully C, Sanz M. Dental Implants in the Medically Compromised Patient. Journal of Dentistry 2013;41(3) 195-206.
[8] Gomez-de Diego R, Mang-de la Rosa M, Romero-Pérez MJ, Cutando-Soriano A, Lopez-Valverde-Centeno A. Indications and Contraindications of Dental Implants in Medically Compromised Patients: Update. Medicina Oral Patologia Oral y Cirugia Bucal 2014;19(5):e438, -9.
[9] Preoteasa E, Murariu CM, Ionescu E, Preoteasa CT. Acrylic Resin Reinforcement With Metallic and Nonmetallic Inserts. Revista Medico-Chirurgicala a Societatii de Medici si Naturalisti din Iasi 2007; 111(2) 487-93.
[10] Lerner H. Minimal invasive implantology with small diameter implants. Implant Practice 2009, 2(1) 30-5.
[11] Preoteasa E, Meleşcanu-Imre M, Preoteasa CT, Marin M, Lerner H. Aspects of oral morphology as decision factors in mini-implant supported overdenture. Romanian Journal of Morphology and Embryology 2010;51(2) 309-14.
[12] Shatkin TE, Shatkin S, Oppenheimer AJ, et al. A simplified approach to implant dentistry with mini dental implants. Alpha Omega. 2003; 96(3) 7-15.
[13] Preoteasa E, Imre M, Preoteasa CT. A 3-Year Follow-up Study of Overdentures Retained by Mini–Dental Implants. The International Journal of Oral & Maxillofacial Implants 2014; 29(5) 1034-41.
[14] Sohrabi K, Mushantat A, Esfandiari S, Feine J. How successful are small-diameter implants? A literature review. Clinical Oral Implants Research 2012;23 (5) 515–525.
[15] Block MS1, Delgado A, Fontenot MG.The effect of diameter and length of hydroxylapatite – coated dental implants on ultimate pullout force in dog alveolar bone. Journal of Oral and Maxillofacial Surgery 1990;48(2) 174-8.
[16] Renouard F, Nisand D. Impact of implant length and diameter on survival rates. Clinical Oral Implants Research 2006;17 (2) Supplement 35-51.
[17] Singh RD, Ramashanker, Chand P. Management of atrophic mandibular ridge with mini dental implant system. National Journal of Maxillofacial Surgery 2010;1(2) 176-8.
[18] Griffitts TC, Collins CP, Collins PC. Mini dental implants: an adjunct for retention, stability, and comfort for the edentulous patient. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 2005;100 (5) 81-4.
[19] Misch CE. Contemporary Implant Dentistry 2nd edition. St. Louis: Mosby Inc; 1999.
[20] Rossein KD. Alternative treatment plans: implant supported mandibular dentures. Inside Dentistry 2006; 2(6) 42-43.
[21] Melescanu Imre M, Preoteasa E, Tancu A, Preoteasa CT. Imaging Technique for the Complete Edentulous Patient Treated Conventionally or With Mini Implant Overdenture. Journal of Medicine and Life 2013;6(1) 86-92.
[22] Campelo LD, Camara JR. Flapless implant surgery: A 10-year clinical retro- spective analysis. International Journal Oral Maxillofacial Implants 2002;(17) 271–276.
[23] Sunitha RV, Sapthagiri E. Flapless implant surgery: A 2-year follow-up study of 40 implants. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2013;116 (4) 237–243.
[24] Scherer MD, Ingel AP, Rathi N. Flapped or Flapless Surgery for Narrow-Diameter Implant Placement for Overdentures: Advantages, Disadvantages, Indications, and Clinical Rationale. The International Journal of Periodontics & Restorative Dentistry 2014;34(3) Supplement 89-95.
[25] Christensen GJ.The ‘mini’-implant has arrived. The Journal of the American Dental Association 2006;137(3) 387-90.
[26] Preoteasa E, Iosif L, Amza O, Preoteasa CT, Dumitrascu C. Thermography, an Imagistic Method in Investigation of the Oral Mucosa Status in Complete Denture Wearers. Journal of Optoelectronics and Advanced Materials 2010;12(11) 2333–4.
[27] Awad MA, Lund JP, Dufresne E, Feine JS. Comparing the efficacy of mandibular implant-retained overdentures and conventional dentures among middle-aged edentulous patients: satisfaction and functional assessment. The International Journal of Prosthodontics 2003;16, 117–22.
[28] Flanagan D, Mascolo A. The Mini Dental Implant in Fixed and Removable Prosthetics: A Review. Journal of Oral Implantology 2011;37 (1) 123-132
[29] Bulard RA. Mini implants. Part I. A solution for loose dentures. The Oklahoma Dental Association Journal. 2002;93.42-46.
[30] Dantas Ide S, Souza MB, Morais MH, Carreiro Ada F, Barbosa GA. Success and survival rates of mandibular overdentures supported by two or four implants: a systematic review, Brazilian Oral Research 2014;28(1) 74-80.
[31] Bergendal T, Engquist B. Implant-supported overdentures: a longitudinal prospective study. The International Journal of Oral & Maxillofacial Implants 1998;13 (2) 253–62.
[32] Klein MO, Schiegnitz E, Al-Nawas B. Systematic review on success of narrow-diameter dental implants. The International Journal of Oral & Maxillofacial Implants. 20







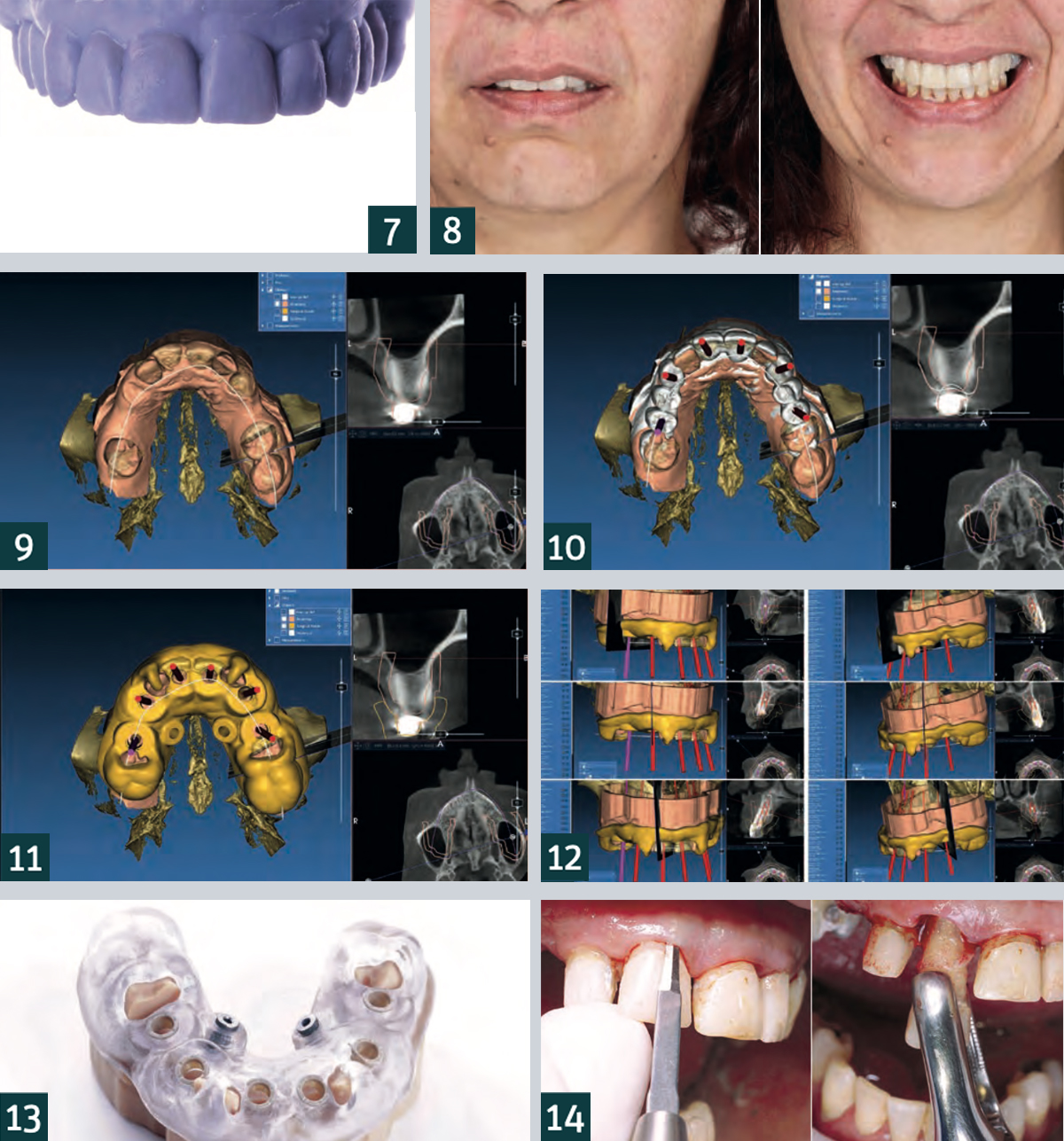
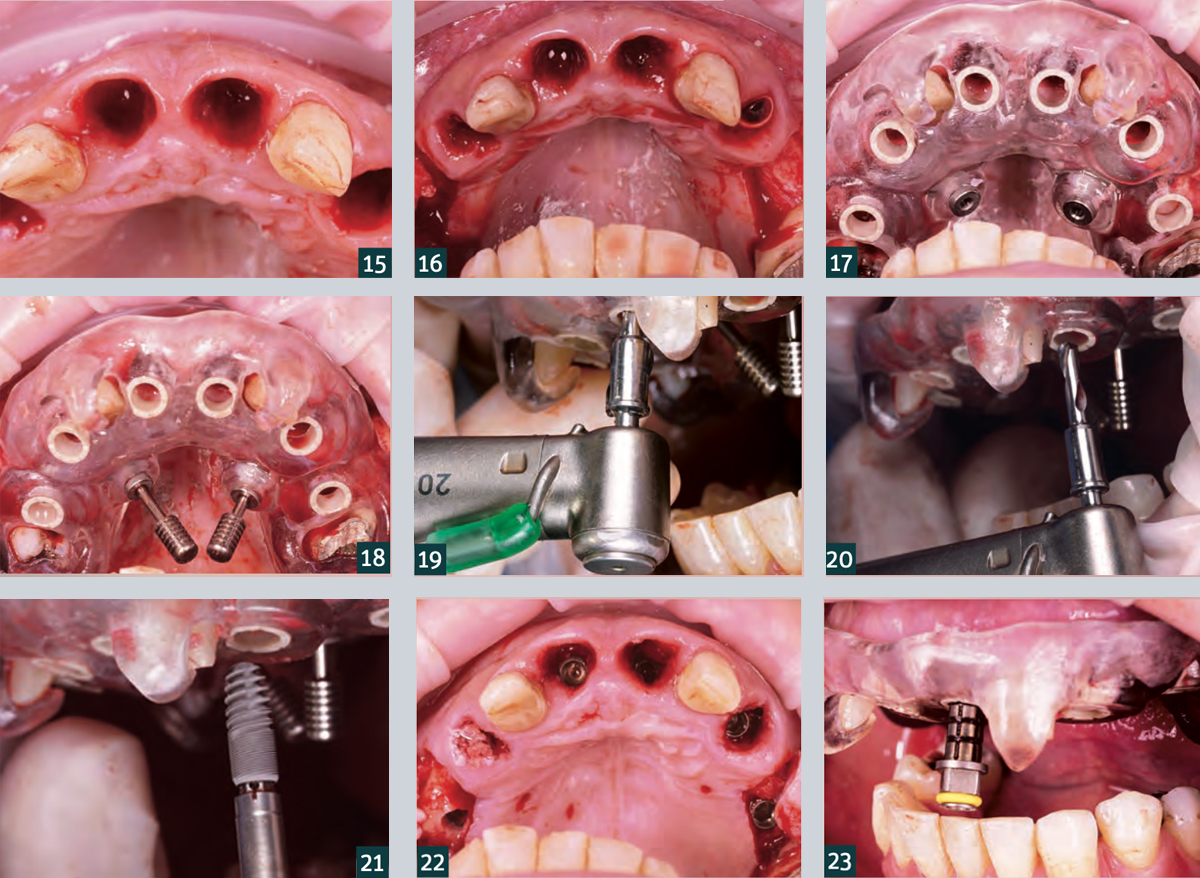 15. Teeth 12 and 22 were initially left in place to stabilise the surgical guide.
15. Teeth 12 and 22 were initially left in place to stabilise the surgical guide.